Liposuction Treatment Areas at Venus Clinic
In this section, we present the liposuction treatment areas available at Venus Clinic, along with before-and-after photographs. Certain body areas are typically treated together as a unit during liposuction. Understanding these anatomical relationships will help you determine which areas would benefit most from treatment.

1. Trunk Liposuction
CIRCUMFERENTIAL THORACOABDOMEN
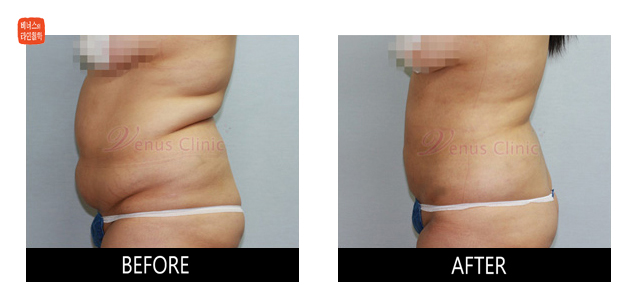
The abdomen is the most commonly requested liposuction area for both men and women, and one of the most rewarding in terms of patient satisfaction.
Because the abdomen presents a wide, flat surface, it is essential to remove fat evenly while leaving a thin, uniform layer of subcutaneous fat to achieve a smooth result.
The lower abdomen has two distinct fat layers. Within the superficial fascial system, the lower abdominal structure is uniquely named Scarpa's fascia, which divides the fat into superficial and deep layers. In adults, the deep layer thickens over time, causing the lower abdomen to protrude. Therefore, thorough removal of this deep layer during liposuction is essential to prevent fat recurrence. Fortunately, even loose or wrinkled lower abdominal skin contracts well after surgery, yielding excellent results without the need for skin excision.
Unlike the lower abdomen, the upper abdomen consists of a single fat layer comprising an areolar (mesh-like) superficial component and a lamellar (layered) deep component. Due to fibrous fascial adhesions to the skin near the waist and the prominence of the rib cage, complete fat removal in the upper abdomen can be challenging. The upper abdomen also contains more fibrous tissue than the lower abdomen, which can lead to increased bleeding during surgery.
After surgery, skin retraction in the upper abdomen is less pronounced than in the lower abdomen, which may result in residual skin laxity or a slightly protruding appearance. Additionally, unlike the lower abdomen, the upper abdomen can flex and form horizontal creases that may be mistaken for residual fat -- an important distinction to understand. If fat removal is incomplete, revision surgery may occasionally be necessary.
The flanks are generally composed of two or more fat layers, particularly in the posterior and paralumbar regions. Excess calories are converted to fat and stored primarily in the deep layer, which is why the waistline gradually disappears with age. Thorough and precise suctioning in the prone position consistently produces excellent results in this area.
The fat layer overlying the rib cage is positioned on the chest when lying down, but shifts downward due to gravity when standing, causing sagging and wrinkling as it descends to the abdominal area. Since liposuction is performed in the supine position, neglecting the chest wall fat above the ribs will result in it hanging into the abdominal zone postoperatively, compromising the overall result. The deep layer in this region is rich in fibrous tissue, and muscles wrap around the ribs, creating a risk of muscle injury and bleeding if fat tissue is misidentified.
The waistline region and the subscapular back (where the bra line crosses) are areas where fat accumulation sags in the standing position, potentially creating folds at the waist. Removing the fat in these areas during abdominal liposuction is essential for achieving a complete, attractive waistline and back contour.
Venus Clinic's thoracoabdominal liposuction includes the chest area above the ribs, the waistline region, and the subscapular back in addition to the full abdomen. By removing fat layers that sag toward the abdomen when standing, this approach creates a natural S-line silhouette for patients with typical upper-body obesity. Even patients who naturally lack a defined waist indentation can achieve an attractive waistline through this procedure.


UPPER / LOWER ABDOMEN
The upper abdomen is particularly prominent in patients with significant visceral obesity, more commonly seen in men. These patients often experience postprandial bloating, which typically improves considerably after liposuction. The lower abdomen is a common concern for women, especially those with abdominal wall laxity following childbirth. Fortunately, skin retraction after lower abdominal liposuction is excellent, producing outstanding results without surgical skin excision. The lower abdomen remains one of the highest-satisfaction treatment areas.
WAIST / MALE FLNAK(LOVE HANDLE)/ HIP
In women, the lateral silhouette of the waist and flanks typically forms a natural S-curve, while in men it tends to be more linear. With aging, fat accumulates in these areas and proves resistant to diet and exercise -- often referred to as "age-related fat." For patients without severe overall abdominal obesity, liposuction of just the hips, waist, and flanks can restore the youthful S-line silhouette.

FLANK
When wearing light clothing in summer, bulges along the bra line above and below are commonly visible. This is typically caused by hypertrophy of the fat layer above the flanks over the rib cage. Treating this area together with the upper back produces highly satisfying results.

BACK
The back is one of the most challenging areas for liposuction. Dense fibrous tissue and thick skin make fat removal difficult and physically demanding, while limited postoperative skin retraction can make it hard to achieve fully satisfying results. For this reason, laser or ultrasound energy is sometimes used to emulsify the fat before suctioning.
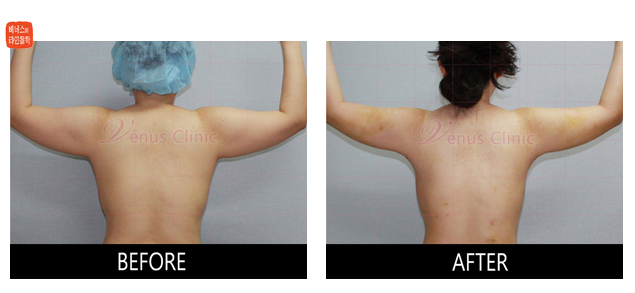
The ideal feminine back differs from the masculine inverted-triangle shape. In women, a near-90-degree angle between the arms and the torso is considered most attractive, which requires smooth contouring of the axillary and lateral back regions.
2. Upper Body Liposuction
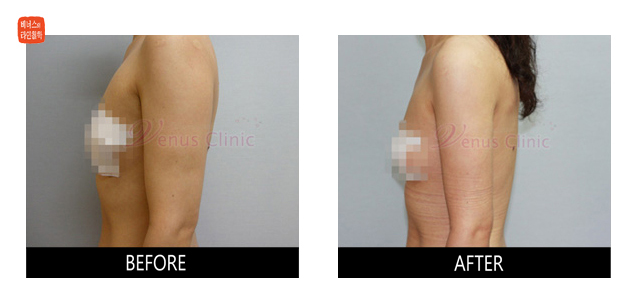
CIRCUMFERENTIAL ARM / AXILLA / BACK
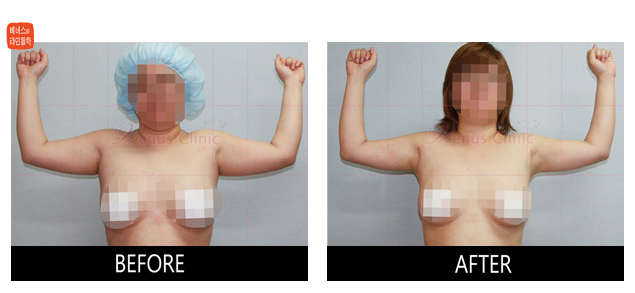
The arms are one of the most rewarding areas for liposuction, consistently delivering excellent results and high patient satisfaction. Because arm fat is notoriously resistant to exercise, liposuction is a highly sought-after solution for this area.
What does a beautifully proportioned feminine arm look like? It is slender and taut, without sagging. Specifically, there should be no laxity beneath the biceps on the inner arm, and the outer contour from below the deltoid muscle to the elbow should form a straight, clean line at attention. The anterior axillary fold (the tissue visible in front before the chest contour begins) should not protrude, and the axillary area itself -- where some women may have accessory breast tissue -- must be free of excess fat to maintain a sleek arm silhouette.
Finally, the posterior elbow region -- the lower back of the arm -- is a key area of fat accumulation. A smooth contour here completes the overall feminine line and creates a natural transition to the forearm below.
While liposuction removes fat between the skin and muscle layers and cannot alter bone or muscle structure, it can effectively create a more feminine silhouette through simple fat removal. Unlike dieting, liposuction also induces postoperative skin retraction in the arms, delivering an additional cosmetic benefit.
LATERAL ARM
A prominent lateral arm contour tends to appear more masculine. Moreover, the deltoid muscle overlies this area, so some of the bulk may be muscular rather than adipose, potentially limiting the degree of size reduction achievable.
However, even removal of a small amount of fat can dramatically feminize the lateral arm silhouette by creating a straight, clean outer line. Care must be taken below the deltoid, where excessive suctioning can create an unnatural concavity.

POSTERIOR ARM
The posterior arm is the area most commonly requested by patients seeking arm liposuction, and it yields the most dramatic improvement. Thorough fat removal in both the axillary and elbow regions is essential for achieving a beautifully straight arm contour. Incomplete removal can result in residual sagging or a club-shaped arm appearance.
In patients with well-developed biceps and triceps, the change in arm circumference may be modest, or some residual laxity may persist. Since the posterior arm is contiguous with the axillary area, combining it with posterior axillary and back liposuction produces significantly better results.
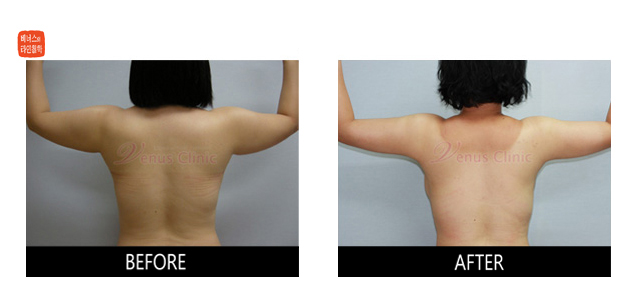
ANTERIOR POSTERIOR SIDE OF THE AXILLA
Many patients who initially undergo arm liposuction alone later return to address the anterior and posterior axillary folds, sometimes called "bra fat." The anterior axillary fold -- the tissue between the axilla and the breast -- contains relatively little fat but prominently frames the front of the chest, so its removal produces a noticeable improvement.
The posterior axillary area overlying the upper scapular back produces dramatic results when treated together with the posterior arm. This region transforms the torso silhouette from an inverted triangle to a straighter line when the arms are raised. In men, a 90-degree arm elevation creates an obtuse angle at the axilla, emphasizing a muscular, triangular upper body. In women, a straight-line contour at 90 degrees is considered the ideal silhouette.
Combining arm liposuction with posterior axillary back liposuction creates a feminine upper body contour from behind, widens the gap between the arm and torso to reduce skin friction, and significantly diminishes the bulges visible at the posterior arm and axilla when standing at attention.
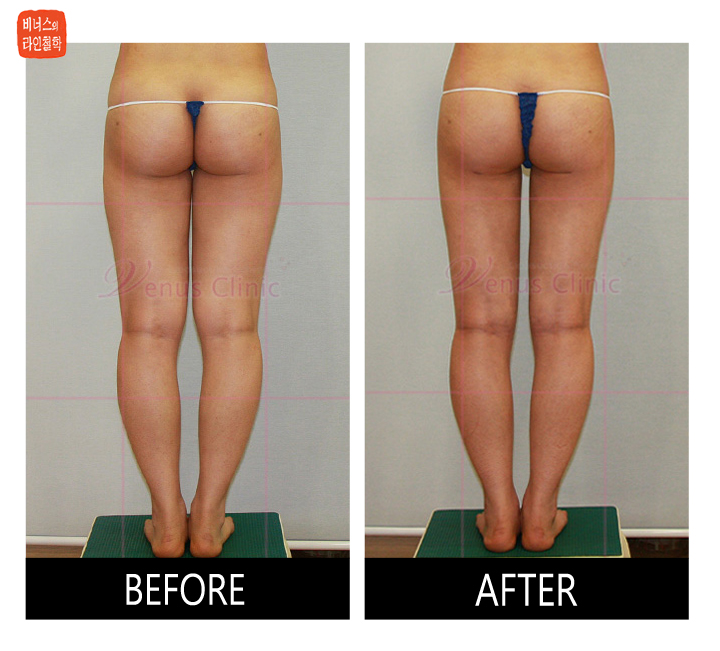
3. Lower Body Liposuction
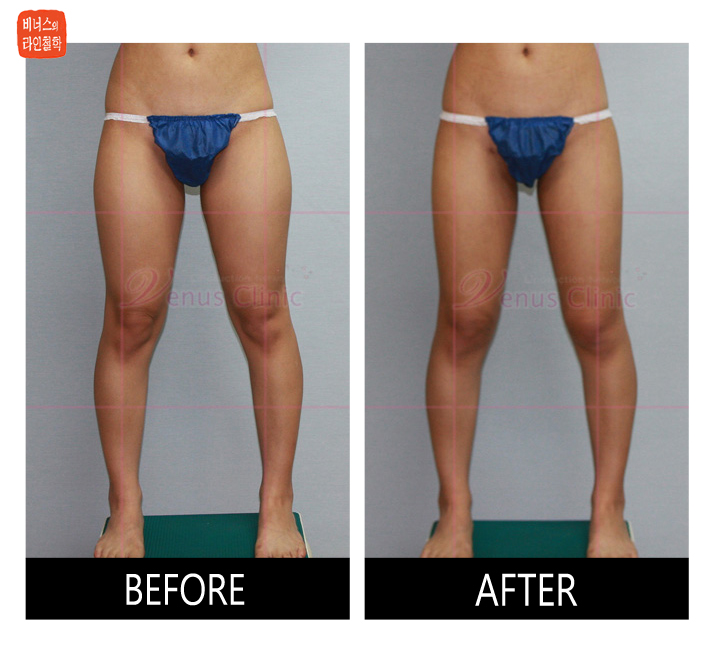
CIRCUMFERENTIAL THIGH / BUTTOCK / HIP/ KNEE
Compared to other body areas, the thighs show little improvement from diet, exercise, or other weight loss efforts. They are often the last area to slim down even as the rest of the body loses weight, which can be a persistent source of frustration.
Many patients find themselves wearing different clothing sizes for the upper and lower body due to disproportionately full thighs -- a condition sometimes called "Two Body Syndrome," or pear-shaped body type. For these individuals, liposuction can create a slender, attractive lower body contour.
Because the thigh is a cylindrical structure, fat must be removed evenly around its full circumference with an aesthetic sensibility to achieve a favorable outcome that is well-balanced with the rest of the body.
The outer thigh is typically treated together with the adjacent lower outer buttock area, which naturally addresses the lateral bulging caused by the weight of the buttocks above.
The inner thigh requires particular care and precision. The upper inner thigh contains fat tissue with relatively little fibrous support, giving it a soft, jelly-like consistency that is suctioned easily and rapidly. This increases the risk of over-removal, which can result in surface irregularities. Using tumescent anesthesia and microcannulas ensures consistent, smooth results. The anterior thigh has relatively uniform subcutaneous fat with minimal fibrous resistance, making it easy to traverse. Care must be taken to avoid excessive suctioning and to preserve smooth, natural contours.
Treating the entire circumferential thigh in a single session carries a higher complication risk than staged procedures. However, with proper application of the tumescent technique, appropriate fat removal volumes, and comprehensive postoperative care, patients can achieve a well-balanced lower body in a single treatment with full recovery.
In young women, the buttocks form a smooth, dome-shaped contour. As fat accumulates, the buttocks enlarge and may become irregular. With aging, the lower lateral buttocks expand and the supporting ligaments stretch, leading to natural ptosis (sagging). When the buttocks are excessively large, the goal of liposuction is to reduce size and volume while maintaining a natural, symmetrical shape that remains proportional to the thighs.
For patients with typical lower body obesity, simultaneous liposuction of the circumferential thighs, buttocks, and knees is recommended to achieve a harmonious hip-buttock-thigh contour. The procedure should be approached three-dimensionally, emphasizing curves over straight lines to enhance the feminine figure.
Venus Clinic pursues overall balance with maximum size reduction by removing an adequate volume of fat. We typically perform simultaneous liposuction of the full 360-degree circumferential thighs, knees, buttocks, and hips in a single session. We recommend treating the complete aesthetic unit so that even if weight is regained in the future, the evenly reduced fat layer maintains a proportional shape without distortion.
This comprehensive approach allows simultaneous creation of the outer contour from hip to knee, buttock narrowing and lifting, the posterior buttock line, the anterior thigh line from groin to knee, and the inner line from the medial thigh through the knee to the calf. The result is a fully balanced lower body. Achieving beautiful results requires both volume reduction and preservation of feminine curves -- a combination that demands artistic sensibility, extensive liposuction experience, and strong physical endurance on the part of the surgeon.


ANTERIOR THIGH
For patients who complain of thick thighs, the anterior thigh is typically the area with the greatest fat accumulation. In men, this region tends to be thicker due to muscular development, while in women, it is rich in adipose tissue and responds exceptionally well to liposuction. Treatment of the anterior thighs can noticeably reduce clothing size and create a more slender thigh contour.
MEDIAL THIGH
The medial thigh is another highly requested area among women. This region is prone to perspiration, especially during menstruation or in summer, and the constant skin-to-skin contact can cause chafing, irritation, and even lichenification (darkening of the skin).
Because the medial thigh fat contains relatively little fibrous tissue, it suctions easily -- but this also increases the risk of creating depressions or irregularities if not performed with great care. Treating the medial thigh together with the inner knee creates a straight inner leg line from thigh to calf, making the legs appear longer.

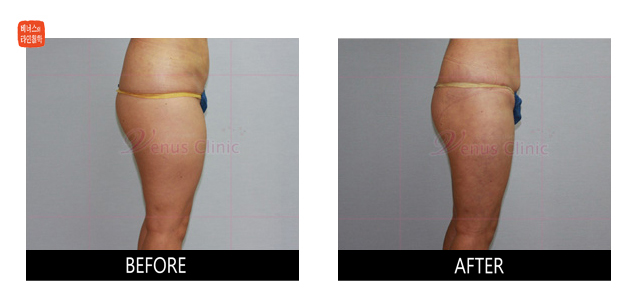
SADDLE BAG
The lateral thigh, or "saddlebag" area, is a uniquely feminine fat deposition site. Because this fat accumulation is hormonally driven, it responds poorly to dieting and even to injectable fat-dissolving treatments. Saddlebags cause the outer thigh to bulge when wearing jeans, detracting from the overall appearance and making the legs appear shorter.
When accompanied by significant fat accumulation on the outer buttocks, the weight of the buttocks exacerbates the lateral bulging. In such cases, combining buttock liposuction with saddlebag treatment produces a more effective and aesthetically pleasing result. However, standalone saddlebag mini-liposuction is also frequently performed.

HIP / BUTTOCK / LATERAL THIGH
The hip, buttock, and lateral thigh together constitute a single cosmetic unit. The outer contour from the upper hip (just below the waist) through the buttocks and down the lateral thigh -- along with the breasts -- represents the quintessential symbol of feminine beauty. Simultaneous liposuction of all three areas is therefore essential for creating a beautifully feminine body line.
Removing fat from the outer and lower portions of the buttocks causes the buttock tissue to centralize and lift, creating the appearance of longer legs. This is commonly called the "hip-up effect" (more accurately, the "buttock-up effect"), as the previously sagging buttocks take on an uplifted, aesthetically appealing contour.

KNEE
Knee liposuction is one of the most effective and rewarding procedures. Removing the protruding fat pad on the inner knee creates a straight inner contour from the thigh to the calf, making the legs appear longer and producing a beautiful "mini-skirt line."
While inner knee liposuction can be performed together with medial thigh or calf liposuction, excellent results are achievable with knee liposuction alone. However, satisfying outcomes require meticulous, thorough fat removal.
Most clinics do not include the knee region in standard thigh liposuction. At Venus Clinic, we typically include the bilateral hip area above the buttocks for a seamless hip contour and extend downward to include the knees, creating a smooth, continuous thigh-to-calf transition.

CIRCUMFERENTIAL LEG
Uneven or aesthetically unfavorable fat distribution in the calves is genetically determined and generally does not respond to diet or exercise.
The calf is considered one of the most technically challenging areas for liposuction. It consists of only a single fat layer requiring precise surgical technique. The leg silhouette is primarily determined by the calf and ankle musculature, so photographic improvement may appear less dramatic. Few patients have prominently bulging focal fat deposits, the curved anatomy makes suctioning difficult, incision sites are more visible, postoperative swelling persists longer, recovery is slower, and patient expectations tend to be high -- all of which contribute to the difficulty of this procedure.
With accurate assessment of calf muscle development and fat layer thickness, meticulous liposuction using microcannulas can produce satisfying results. However, excessive suctioning can expose the underlying muscle contour, creating a masculine, muscular-looking calf.
Patients with thick ankles or bow-legged appearance can benefit from targeted ankle liposuction and lateral calf suctioning. Prolonged standing after calf surgery can cause persistent swelling and discomfort, so patients should elevate their legs above heart level when standing for extended periods. It is important to note that thick ankles are frequently caused by edema related to internal medical conditions rather than excess fat, so preoperative consultation is essential.
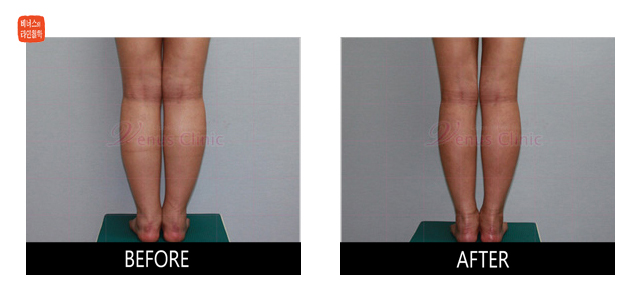
<Case of calf liposuction after the thigh liposuction>
4. Chin and Face Liposuction
CHIN / CHEEK /JOWL
With aging, fat accumulates beneath the chin and skin elasticity declines, resulting in a double chin and loss of a defined jawline. Tumescent liposuction is the most effective method for submental fat removal, particularly for patients who wish to avoid the prolonged recovery, scarring, and potential side effects associated with surgical facelifts.
The chin and jowl areas are among the most rewarding regions for liposuction, addressing a common sign of aging typically seen in the 40s and 50s. Fat is removed only from the superficial layer above the platysma muscle -- the neck muscle visible when clenching the jaw. Fat beneath the platysma cannot be treated due to the risk of injury to the airway, nerves, and blood vessels. Using microcannulas ensures smooth results without surface irregularities. To promote skin retraction in lax skin, laser or VASER ultrasound energy may also be applied. Extreme care must be taken to avoid facial nerve and vascular injury, which could cause not only bleeding but also facial muscle paralysis.
For patients with significant chin skin laxity, third-generation ultrasound-assisted (VASER) liposuction or Nd-YAG laser application within the fat layer may be used prior to suctioning to promote enhanced skin retraction.

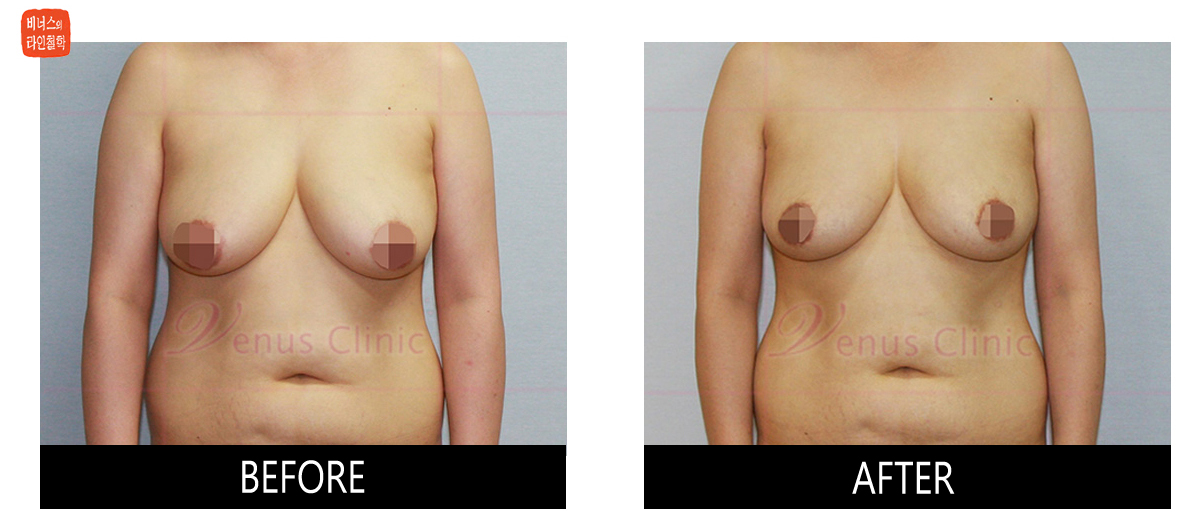
5. Breast Liposuction
BREASTS
Many women experience significant discomfort and distress due to excessively large breasts. The weight of the breasts can cause pain, restrict daily activities, and create considerable psychological stress. Over time, breast weight leads to postural changes and chronic degenerative pain in the neck, shoulders, and back. Bra straps leave indentations and may cause skin irritation or dermatitis, and even expensive clothing does not fit properly.
Liposuction is an effective solution for these concerns. Female breast liposuction is performed under local anesthesia using specialized microcannulas (2 mm diameter) to reduce breast volume without visible scars. The procedure involves virtually no postoperative pain and allows rapid recovery with an easy return to daily life. Removing 30 to 50% of breast fat produces no lasting side effects, and most patients resume normal activities within 2 to 3 days.
Conventional surgical breast reduction requires general anesthesia and involves lengthy operative time, significant postoperative pain, prominent scars, and an extended recovery period. By contrast, liposuction-based breast reduction decreases breast size proportionally to the volume of fat removed, effectively restores the supporting ligament function to lift the breast, and elevates both the nipple position and the inframammary fold.
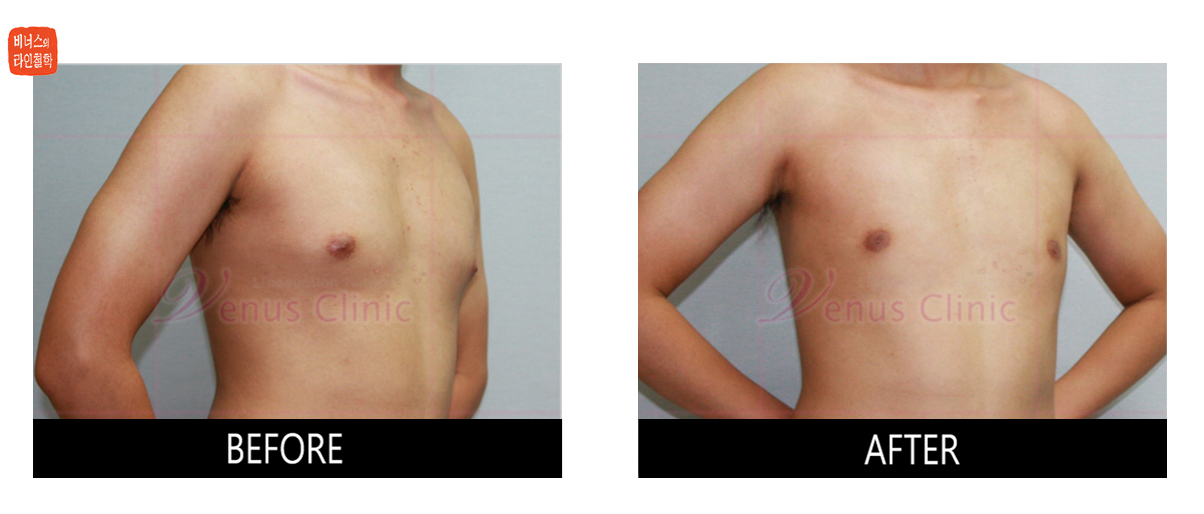
GYNECOMASTIA
Gynecomastia -- the enlargement of male breast tissue -- has become increasingly common alongside rising obesity rates. In most cases, the condition results from increased fat deposition in the breast area. Gynecomastia is defined as the overdevelopment of glandular breast tissue and/or adipose tissue in males. While the most common cause is obesity, other contributing factors include hormonal imbalances, medications, and hormone-producing tumors.
Unilateral breast enlargement in men, though rare, may be associated with male breast cancer and warrants thorough clinical investigation.
Gynecomastia is classified into three types:
- Pseudogynecomastia (fatty type): Normal glandular tissue with excess fat deposition only. This is most commonly associated with obesity.
- True gynecomastia (pure type): Glandular tissue proliferation causing breast enlargement. The size and shape may closely resemble a female breast.
- Mixed type: A combination of both glandular tissue proliferation and excess fat deposition.
In most cases of pseudogynecomastia, no specific underlying cause can be identified. It is important to distinguish between normal and abnormal male breast development. While breast tissue is generally not palpable in normal males, gynecomastia measuring less than 4 to 5 cm in diameter may still fall within normal limits.
Pathological gynecomastia can arise from the following mechanisms:
- 1. Testosterone deficiency or functional impairment (congenital anorchia, Klinefelter syndrome, testicular feminization syndrome)
- 2. Increased estrogen production (abnormal chorionic gonadotropin secretion by testicular or bronchogenic carcinoma; estrogen production in true hermaphroditism)
- 3. Increased peripheral conversion of androgens to estrogen (congenital adrenal hyperplasia, hyperthyroidism, feminizing adrenal tumors). Of particular note, anabolic steroid use can induce gynecomastia; in Korea, some herbal medicines may contain steroid compounds, which can lead to recurrence even after surgical treatment.
- 4. Medications (digitalis, alkylating agents, spironolactone, cimetidine, busulfan, isoniazid, tricyclic antidepressants, D-penicillamine, anabolic steroids, phenytoin, clomiphene, diazepam, heroin, marijuana)
- 5. Post-traumatic
Gynecomastia can be effectively treated with liposuction, which produces no visible scars and delivers excellent results with high patient satisfaction. In cases with excessive glandular tissue, surgical excision through a small incision may be necessary.
Recent reports have demonstrated that VASER (third-generation ultrasound-assisted liposuction) is effective for gynecomastia treatment by disrupting glandular tissue and emulsifying fat prior to suctioning, and also promotes significant skin retraction in cases with marked skin laxity.
Patients can resume daily activities the day after surgery, with virtually no restrictions by two weeks. A compression garment should be worn for approximately one month to promote tissue adherence. Final results are typically evident at two months. Temporary altered sensation may occur but is transient, resolving within 2 to 3 months.